Several bills impacting healthcare and hospitals were advanced through committees in the state Senate during the week of Oct. 28. The Senate Health Policy Committee unanimously approved Senate Bills (SB) 916 – 918, led by Sen. …
The MHA Legislative Policy Panel held their first meeting of the MHA program year at the MHA Capital Advocacy Center Oct. 30 to develop recommendations on legislative issues impacting Michigan hospitals. Chad Tuttle, SVP, clinical …
The MHA Service Corporation (MHASC) board met Oct. 24 to discuss healthcare market strategies to identify, diversify and grow solutions for MHA members and clients. The board retreat focused on how the MHASC can support …
The MHA hosted a webinar Oct. 23 overviewing the National Special Pathogen System (NSPS) of care. The NSPS is a tiered system with four facility levels that have increasing capabilities to care for suspected …
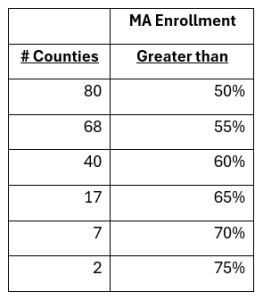
The MHA updated its analysis of Medicaid and Medicare enrollment based on September 2024 data. The analysis includes program enrollment as a percentage of each county’s total population and the split between fee-for-service and …
The MHA will host the webinar How Boards and Leaders Can Deploy AI Responsibly and Ethically, scheduled 4:30 – 6 p.m. ET, Dec. 3. The webinar will cover a framework to govern the approach, policies and procedures …
Keckley Report
 Looking to 2025: The Stop-Gap Actions likely on Healthcare’s 8 Most Urgent Issues
Looking to 2025: The Stop-Gap Actions likely on Healthcare’s 8 Most Urgent Issues
“Last week, I wrote about three predictions for healthcare regardless of next week’s the election results:
- States will be the epicenter for healthcare legislation and regulation; federal initiatives will be substantially fewer.
- Large employers will take direct action to control their health costs.
- Private equity and strategic investors will capitalize on healthcare market conditions.
As these play out, eight major issues will get attention vis a vis stop-gap measures reflecting regulator and elected officials’ responsiveness to industry pressure and voter sentiment …
These issues are not new to healthcare: they’ve prompted endless symposia, sponsored white papers and discussion by trade associations, special interests and think tanks offering solutions beneficial to preserving their view of what’s needed. What’s new is the public’s distaste for the status quo in healthcare: in every major poll conducted since the pandemic, trust and confidence in the health system has been low and majorities have said the status quo is unsatisfactory.
Thus, stop-gap measures serve two purposes: they enable elected officials and government agency personnel to demonstrate responsiveness to important issues and they provide foundations for additional rules, laws and actions downstream. They’re a start.”
Paul Keckley, Oct. 28, 2024
The general election is Tuesday, Nov. 5. Polls open at 7 a.m. and close at 8 p.m. Voters in line at 8 p.m. can still cast ballots. The MHA strongly encourages voter participation, knowing those …
Becker’s Hospital Review published an article Oct. 31 that includes responses from MHA CEO Brian Peters and other MHA members. Becker’s asked C-suite executives from hospitals and health systems across the U.S. to share their …






 Looking to 2025: The Stop-Gap Actions likely on Healthcare’s 8 Most Urgent Issues
Looking to 2025: The Stop-Gap Actions likely on Healthcare’s 8 Most Urgent Issues